![]()
Download Latest EFM Dumps with Authentic Real Exam Questions
Authentic EFM Exam Dumps PDF - Mar-2026 Updated
NEW QUESTION # 45
An internal electronic fetal monitor tracing continues to record artifact despite equipment troubleshooting and replacement of the spiral electrode. The next action is to:
- A. Provide oxygen
- B. Auscultate the fetal heart rate
- C. Reposition the woman
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
When internal monitoring continues to record artifact despite:
* Changing the scalp electrode
* Ensuring correct attachment
* Checking cable connections
* Confirming maternal movement is not the cause
NCC requires confirmation of fetal well-being using another modality.
The correct next step is direct auscultation with Doppler or fetoscope.
Why other answers are incorrect:
* Oxygen is not indicated for equipment malfunction.
* Repositioning does not resolve internal FHR artifact.
Thus, Auscultate the fetal heart rate is the appropriate next step.
References:NCC C-EFM Candidate Guide; AWHONN; Miller's Pocket Guide; Menihan.
NEW QUESTION # 46
A woman at 38-weeks gestation is admitted to labor and delivery following a fall down the stairs three hours ago. She started feeling contractions in the ambulance. The fetal heart rate tracing shown is on initial evaluation and represents 25 minutes. This tracing is most consistent with a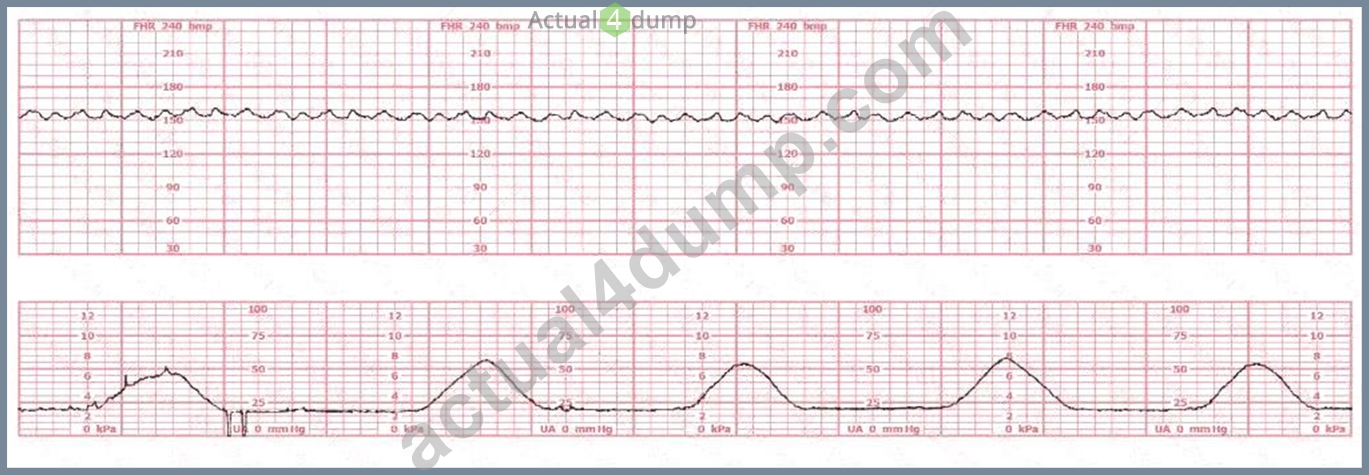
- A. category I tracing
- B. category II tracing
- C. category III tracing
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract without any URL or Links According to the NCC C-EFM 2025 Candidate Guide, Pattern Recognition and Intervention requires the candidate to classify fetal heart rate (FHR) patterns using the NICHD 2008 three-tier system, which NCC endorses across all recommended resources (AWHONN Fetal Heart Monitoring Principles and Practices, Menihan Electronic Fetal Monitoring, Simpson & Creasy, Miller's Pocket Guide).
A Category II tracing is defined as "indeterminate" and includes any FHR pattern that is not Category I and not Category III. NCC references indicate that Category II may include:
* Minimal or marked variability
* Absence of accelerations after fetal stimulation
* Recurrent variable decelerations with moderate variability
* Prolonged decelerations lasting 2-10 minutes
* Baseline tachycardia or bradycardia without absent variability
In the tracing provided:
* The baseline FHR is approximately 135-145 bpm, within normal limits.
* Moderate variability is not consistently present; variability is borderline minimal-moderate at times.
* No significant accelerations are seen over the 25-minute evaluation period.
* No recurrent late or prolonged decelerations are present.
* There are occasional subtle variable-type dips, but not enough to meet criteria for Category III.
NCC-endorsed texts (such as AWHONN and Menihan) state that a tracing with minimal variability for less than 40 minutes and without recurrent decelerations is Category II, as it fails to meet the requirements for Category I (must have moderate variability and accelerations absent decelerations) and lacks the criteria for Category III (must have absent variability with recurrent late decels, recurrent variable decels, bradycardia, or sinusoidal pattern).
Therefore, this pattern is indeterminate, consistent with Category II, and requires continued surveillance and evaluation, which aligns with NCC-recommended clinical decision-making competencies.
NEW QUESTION # 47
(Full question statement)
Recurrent decelerations are defined as occurring with 50% or more of contractions in any window of how many minutes?
- A. 0
- B. 1
- C. 2
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract Without Links:
According to the NCC C-EFM Content Outline and AWHONN Fetal Heart Monitoring Principles, recurrent decelerations are specifically defined as decelerations that occur with #50% of uterine contractions in a
20-30-minute window, but standardized interpretation guidelines used by NCC and ACOG categorize recurrent patterns based on any 30-minute evaluation period.
AWHONN (FHM 6th Ed.) explains that fetal heart patterns must be evaluated over "a sufficiently long segment, typically 30 minutes, to determine whether the pattern is intermittent or recurrent." Menihan & Simpson further emphasize that recurrent decelerations imply a persistent physiologic stressor, requiring systematic evaluation and intrauterine resuscitation. NCC's Candidate Guide ties this rule directly into categorization within Category II and III tracings. Therefore, 30 minutes is the correct standard evaluation interval for determining recurrence.
NEW QUESTION # 48
A fetal heart rate tracing is abnormal. A change in maternal position and oxygen administration do not correct the pattern. Following birth, a fetal cord blood sample is taken:
pH = 7.25
PaCO# = 46 mm Hg
PaO# = 20 mm Hg
HCO# = 22 mEq/L
Base deficit = -4 mEq/L
These results are best interpreted as:
- A. Normal
- B. Hypoxia
- C. Acidosis
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Normal umbilical arterial values per NCC/AWHONN/Menihan:
* pH: 7.20-7.30
* PaCO#: 45-55 mmHg
* HCO#: 20-24 mEq/L
* Base deficit: 0 to -5 (normal to mild respiratory changes)
This sample shows:
* pH 7.25 # normal
* Base deficit -4 # no metabolic acidosis
* HCO# normal
* Slightly elevated PaCO#, consistent with mild respiratory influence but still normal
* PaO# 20 mmHg is normal for cord arterial blood
This profile is not acidotic (acidosis requires pH <7.10 and base deficit #12).
It also does not indicate hypoxia, which would present with metabolic acidosis.
Therefore: Normal.
References:NCC C-EFM Candidate Guide; AWHONN FHMPP; Menihan; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 49
An electronic fetal monitoring factor that best correlates with fetal well-being is:
- A. Absence of decelerations
- B. Baseline heart rate 140-150 bpm
- C. Presence of variability
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
The single best indicator of fetal oxygenation and neurologic integrity is:
* Moderate baseline variability
Variability reflects:
* Normal autonomic regulation
* Adequate fetal oxygenation
* Intact neurologic pathways
Absence of decelerations is helpful but not as predictive.
Baseline FHR (e.g., 140-150) is normal, but baseline alone does not confirm well-being.
Correct answer: C. Presence of variability
References:NCC C-EFM Candidate Guide; AWHONN FHMPP; NICHD Definitions; Simpson & Creehan.
NEW QUESTION # 50
Fetal cardiac output is essentially dependent on the fetal:
- A. Activity
- B. Baroreceptors
- C. Heart rate
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Because the fetal myocardium is immature, it has:
* Limited ability to increase stroke volume
* Limited ability to increase contractility
Therefore, fetal cardiac output (CO) is almost entirely dependent on heart rate.
NCC and AWHONN physiology describe:
* CO = stroke volume × heart rate
* In the fetus, stroke volume is relatively fixed
* Therefore, changes in HR directly affect cardiac output
* Tachycardia # increases CO
* Bradycardia # decreases CO # decreased perfusion and oxygen delivery
Why the other options are incorrect:
* A. Activity does not fundamentally determine CO.
* B. Baroreceptors regulate HR reflexively but are not the primary determinant of cardiac output.
Correct answer: C. Heart rate
References:NCC Physiology Domain; AWHONN FHMPP; Menihan; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 51
Fetal supraventricular tachycardia will often appear on the monitor as
- A. artifact
- B. the same rate as the maternal pulse
- C. half the actual rate
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources NCC-recommended fetal assessment texts emphasize that external Doppler ultrasound may undercount very rapid fetal arrhythmias such as fetal supraventricular tachycardia (SVT). Because Doppler detects mechanical motion rather than electrical activity, the device may record only every other cardiac contraction
, a phenomenon known as "half-counting."
Menihan's Electronic Fetal Monitoring explains that with SVT-often exceeding 200 to 260 bpm-the monitor "may display a fetal heart rate at approximately half the true atrial rate." AWHONN teaching materials affirm that rapid, regular tachyarrhythmias may appear deceptively slower on the external monitor due to Doppler under-sampling. Simpson & Creehan note that half-counting is a recognized technical limitation and may cause clinicians to miss true tachyarrhythmias if internal monitoring is not applied.
In contrast, artifact displays irregular, inconsistent, and non-physiologic deflections. Matching the maternal pulse suggests maternal heart rate misinterpretation, not SVT.
Miller's Pocket Guide also highlights that half-counting is "commonly seen in fetal SVT when using external Doppler due to failure to detect each rapid contraction." Therefore, fetal SVT most commonly appears as half the actual rate on an external fetal monitor.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesMenihan - Electronic Fetal MonitoringSimpson & Creehan - Perinatal NursingCreasy & Resnik - Maternal-Fetal MedicineMiller's Pocket Guide
NEW QUESTION # 52
This tracing reflects: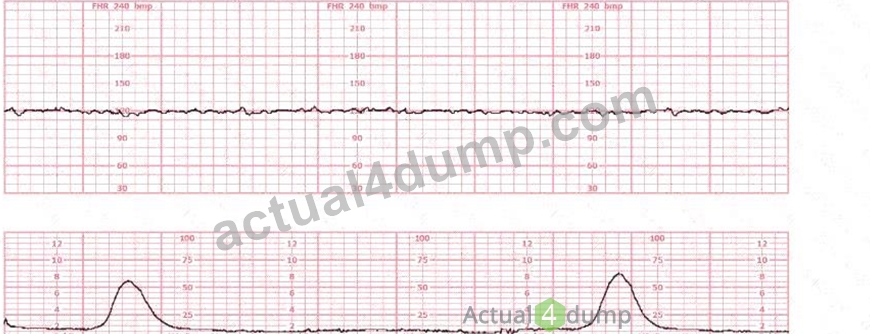
- A. Category III
- B. Category I
- C. Category II
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
In NCC C-EFM interpretation, classification of a fetal heart tracing is based on NICHD's three-tier system:
Category I, II, and III. Category III represents an abnormal tracing requiring immediate evaluation and prompt intervention.
Key findings in this tracing:
* Baseline:Baseline is approximately 140 bpm, within the normal range (110-160 bpm).Baseline alone does not determine category.
* Variability:The tracing shows absent variability:
* No beat-to-beat oscillations
* Flat, minimal fluctuationNICHD and NCC define absent variability as amplitude range undetectable.
* Accelerations:No accelerations are present.
* Decelerations:The strip does not show decelerations or bradycardia.However, absent variability alone with no accelerations for 20 minutes is highly concerning.
Category Classification per NICHD/NCC:
Category III criteria include ANY of the following:
* Absent variability with recurrent late decelerations
* Absent variability with recurrent variable decelerations
* Absent variability with bradycardia
* Sinusoidal pattern
Also recognized as Category III:
* Persistent absent variability lasting #20 minutes with no accelerations, which is strongly suggestive of fetal acidemia when sustained.
This tracing shows:
* Absent variability (flat line)
* No accelerations
* Persisting over an extended period
Under NCC and AWHONN guidance:
A persistently flat tracing must be classified as Category III unless proven otherwise (e.g., fetal sleep, maternal medications), and it requires immediate intrauterine resuscitation and evaluation for potential expedited delivery.
Why Category I is NOT correct:
Category I requires:
* Moderate variability
* No late or variable decelerationsThis tracing does not have moderate variability.
Why Category II is NOT correct:
Category II includes minimal variability, marked variability, intermittent variables/lates, absence of accelerations after stimulation.
This tracing is worse than Category II because variability is absent, not minimal.
Thus, the tracing fits Category III.
References:NCC C-EFM Candidate Guide (2025); NCC Content Outline; NICHD Three-Tier FHR Interpretation System; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 53
This fetal heart rate tracing is of a woman in labor with dichorionic-diamniotic twins at 36-weeks gestation, 4 cm dilated. She is on oxygen via face mask. Based on the fetal heart rate tracing, what is the most appropriate action?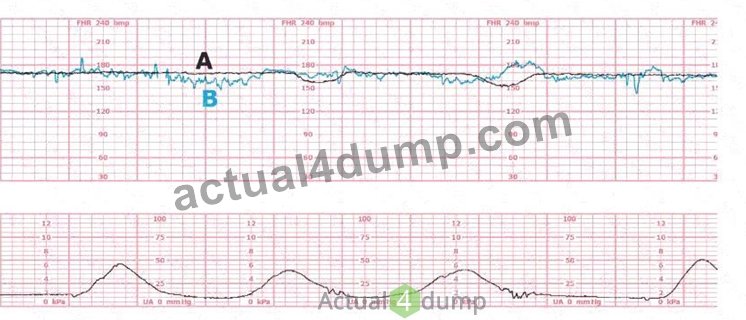
(Tracing A = black; Tracing B = blue)
- A. Give terbutaline
- B. Continue to observe
- C. Cesarean birth
Answer: B
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Both fetal tracings (A and B) show:
* Baselines around 140-150 bpm
* Moderate variability
* Intermittent accelerations
* No recurrent decelerations
* Normal contraction pattern
* Overall Category I patterns for both twins
NCC, NICHD, and AWHONN emphasize that moderate variability with a normal baseline is the strongest reassurance of fetal well-being, even in multifetal gestations.
There is no evidence of:
* Tachysystole
* Recurrent variables
* Recurrent lates
* Prolonged decelerations
* Category III patterns
Therefore, the appropriate action is ongoing observation.
Why the incorrect answers are wrong:
* A. Cesarean birth - Not indicated with Category I FHR patterns.
* C. Terbutaline - Reserved for tachysystole or prolonged deceleration patterns, not present here.
References:NCC C-EFM Candidate Guide; NICHD Definitions; AWHONN FHMPP; Menihan; Simpson & Creehan.
NEW QUESTION # 54
The success of interventions to treat fetal hypoxia first depends on:
- A. Optimizing uteroplacental blood flow
- B. Improving maternal oxygenation
- C. Minimizing uterine activity
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NCC/AWHONN emphasize that the primary goal of intrauterine resuscitation is to:
* Optimize uteroplacental blood flow, which restores fetal oxygen delivery.
Key measures include:
* Maternal repositioning (lateral)
* Reducing tachysystole
* IV fluid bolus
* Correcting maternal hypotension
* Stopping oxytocin
* Treating underlying causes
Improving maternal oxygenation is supportive, but improving uteroplacental perfusion is the critical first determinant of resuscitation success.
Why the other answers are not first priority:
* A. Oxygen - optional and no longer universally recommended unless maternal hypoxemia exists.
* B. Minimizing uterine activity - essential, but still secondary to restoring perfusion.
Correct answer: C. Optimizing uteroplacental blood flow
References:NCC Pattern Recognition & Intervention Domain; AWHONN FHMPP; Menihan; Simpson & Creehan.
NEW QUESTION # 55
This fetal heart rate tracing is from a woman in the second stage of labor. This tracing is best interpreted as: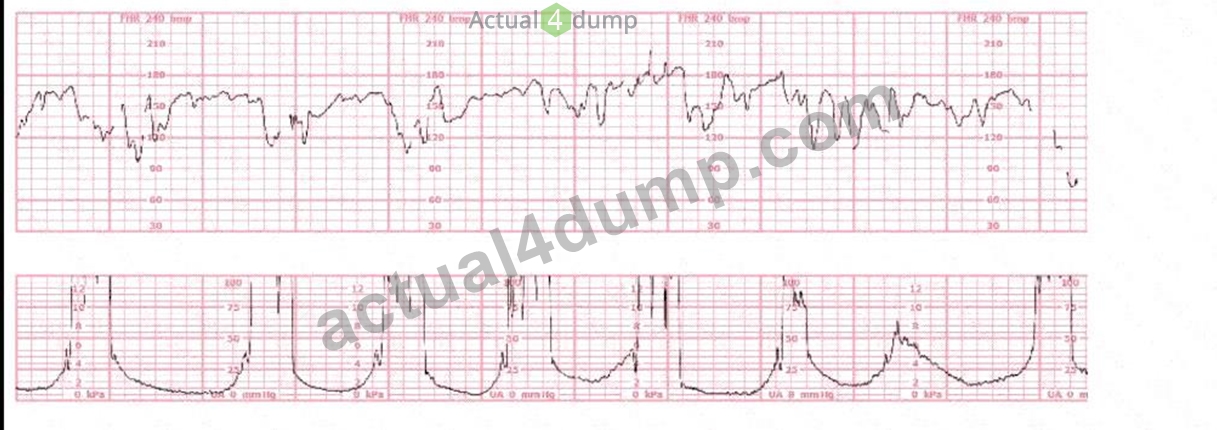
- A. Intermittent late decelerations
- B. Wandering baseline
- C. Variable decelerations
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
The tracing shows the classic features of variable decelerations:
* Abrupt onset (<30 seconds from baseline to nadir)
* Rapid drop followed by a rapid recovery
* Significant variability in shape, depth, and timing
* "Shouldering"-brief accelerations before or after the deceleration, typical of cord compression
* The decelerations vary in appearance and timing relative to contractions In second stage, this pattern is extremely common due to:
* Recurrent cord compression during descent
* Maternal pushing
* Reduced amniotic fluid with advancing labor
Why the other options are incorrect:
A). Intermittent late decelerations
* Late decelerations are uniform, smooth, begin after the contraction peak, and recover after the contraction ends.
* This tracing shows abrupt, variable-shaped, non-uniform decels # NOT late decels.
C). Wandering baseline
* A wandering baseline is a slowly fluctuating, low-amplitude, smooth, preterminal pattern.
* This tracing shows an identifiable baseline with variability and clear decelerations, not wandering baseline.
Thus, the tracing is most consistent with variable decelerations.
References:NCC C-EFM Candidate Guide; AWHONN FHMPP; NICHD FHR Definitions; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 56
To differentiate a fetal dysrhythmia from artifact, it is important to recognize that artifact appears as deflections that are:
- A. Similar in pattern
- B. Uniform but occur irregularly
- C. Varied and disorganized
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Artifact on fetal monitoring:
* Appears erratic, disorganized, and without physiologic pattern
* Shows random amplitude changes
* Often correlates with maternal movement, monitor displacement, or poor signal
* Lacks cyclical, repetitive characteristics seen in true dysrhythmias
Fetal dysrhythmias, by contrast:
* Have repetitive, patterned, predictable rhythm disturbances
* May show uniform premature beats, bigeminy, or sudden rate shifts
Therefore, varied and disorganized = artifact.
References:NCC Candidate Guide; AWHONN FHMPP; Menihan; Miller's Pocket Guide.
NEW QUESTION # 57
The ratio of oxyhemoglobin to the total amount of hemoglobin available is called oxygen
- A. saturation
- B. affinity
- C. carrying capacity
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources Oxygen saturation refers to the percentage of hemoglobin binding sites occupied by oxygen. NCC physiology resources, including Simpson & Creehan and Creasy & Resnik, define oxygen saturation as the
"ratio of oxyhemoglobin to total hemoglobin"-the same definition used in fetal oxygenation discussions.
Oxygen affinity refers to hemoglobin's tendency to bind oxygen (related to the oxyhemoglobin dissociation curve).
Oxygen carrying capacity refers to the total amount of oxygen hemoglobin can transport, independent of current saturation.
AWHONN and Menihan emphasize that fetal oxygenation assessment is dependent on understanding oxygen saturation, not affinity or carrying capacity, when discussing fetal hypoxemia and gas exchange.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesSimpson & Creehan - Perinatal NursingCreasy & Resnik - Maternal-Fetal MedicineMenihan - EFM ConceptsMiller's Pocket Guide
NEW QUESTION # 58
A 45-year-old woman at 36-weeks gestation presents for a nonstress test. Vital signs are: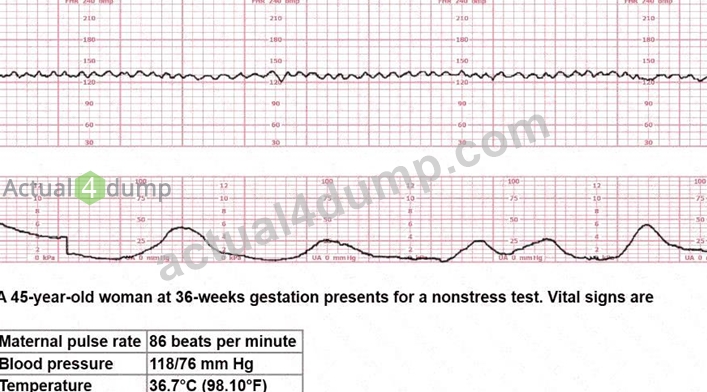
* Maternal pulse rate: 86 beats per minute
* Blood pressure: 118/76 mm Hg
* Temperature: 36.7°C (98.1°F)
The next course of action would include:
- A. Discharge home
- B. Perform a Kleihauer-Betke test
- C. Induce labor
Answer: A
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
The NST strip shows:
* Baseline FHR about 140 bpm
* Moderate variability
* Two or more accelerations meeting 15×15 criteria
* No decelerations
* Normal, infrequent contractions
Per NCC and AWHONN, a reactive NST is defined as:
* #2 accelerations of 15 bpm × 15 seconds in a 20-minute period
* With baseline 110-160 and moderate variability
* No recurrent decelerations
A reactive NST at 36 weeks in a hemodynamically stable mother with normal vitals is reassuring, and the appropriate disposition is routine follow-up and discharge.
Why the other options are incorrect:
* B. Induce labor - Not indicated solely on maternal age or a reactive NST.
* C. Kleihauer-Betke test - Used to quantify fetomaternal hemorrhage after trauma or sensitization risk; there is no such history here.
Therefore, the correct action is A. Discharge home.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 59
A woman at 39-weeks gestation is being induced. She has chronic hypertension controlled by methyldopa (Aldomet). Spontaneous rupture of membranes has occurred; she is 10 cm dilated and at +1 station. The fetal monitor tracing shown is obtained by spiral electrode and tocodynamometer. The next best appropriate action is to: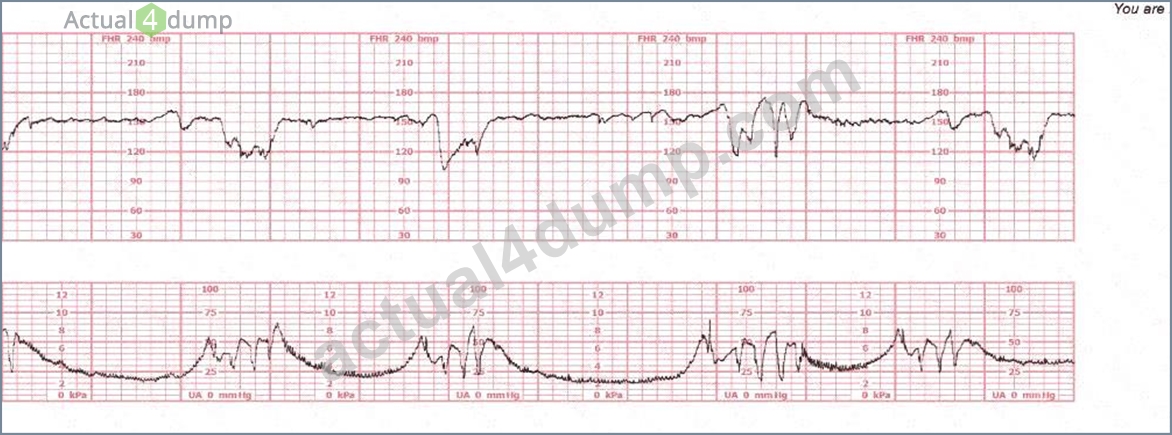
- A. Modify pushing
- B. Consider amnioinfusion
- C. Administer terbutaline
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
The tracing shows recurrent variable decelerations deepening during contractions as the patient is fully dilated and at +1 station.
NCC's Pattern Recognition and Intervention framework states:
* During second stage (complete dilation), variable decelerations commonly occur from cord compression caused by head descent and maternal pushing efforts.
* The FIRST correction for pushing-associated recurrent variable decelerations is modifying the pushing technique:
* Side-lying pushing
* Pushing with every other contraction
* Open-glottis pushing
* Allowing passive descent
These measures relieve head compression and reduce the severity of variable decelerations.
Why the other answers are incorrect
A). Administer terbutaline
* Terbutaline is given for tachysystole with fetal intolerance.
* This tracing does not show tachysystole.
* The pattern is timing-related to pushing, not uterine overstimulation.
B). Consider amnioinfusion
* Amnioinfusion is used for recurrent variable decelerations before complete dilation, when membrane rupture + low fluid is suspected.
* At 10 cm and +1, the fetal head is deep in the pelvis, and the cause of variables is head compression, not cord compression due to oligohydramnios.
* Also, amnioinfusion is impractical and not beneficial at this stage.
Therefore, the correct answer is C. Modify pushing.
References:NCC C-EFM Candidate Guide; NCC Content Outline; AWHONN Principles & Practices; Miller' s Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 60
When the fetal heart rate is measured by a Doppler transducer and the intervals between heart beats are persistently identical, this shows as
- A. normal baseline
- B. absent variability
- C. bradycardia
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources Variability is created by beat-to-beat differences in fetal cardiac intervals due to autonomic nervous system modulation. AWHONN specifies that absent variability appears as "a near-straight line with minimal or no discernible oscillations," which occurs when all beat intervals are identical.
Menihan notes that Doppler displays variability based on mechanical motion and will show flat, unchanging intervals when fetal autonomic modulation is suppressed, reflecting absent variability.
Bradycardia refers to a baseline <110 bpm and does not describe the uniformity of intervals. A normal baseline may still show variability; it cannot have identical beat-to-beat intervals, as this violates the definition of variability in NICHD terminology.
Simpson & Creehan state that absent variability is a significant marker of impaired fetal oxygenation or CNS depression.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesMenihan - Electronic Fetal MonitoringSimpson & Creehan - Perinatal NursingCreasy & Resnik - Maternal-Fetal MedicineMiller's Pocket Guide
NEW QUESTION # 61
This is a tracing of a multiparous woman in the second stage of labor. The vertex is at +3 station. This pattern has continued for the last 20 minutes. She has been pushing for 2½ hours, and oxytocin is infusing at 12 milliunits/minute. Management should include
- A. preparing for cesarean birth
- B. preparing for operative vaginal birth
- C. increasing the oxytocin
Answer: B
Explanation:
Comprehensive and Detailed Explanation (From NCC C-EFM-Referenced Sources) According to NCC C-EFM content guidance and AWHONN Fetal Heart Monitoring Principles (2022), recurrent variable and late patterns in second stage with descent to +2/+3 station require consideration of expediting delivery, especially when maternal effort is prolonged and oxytocin augmentation is already present.
Menihan & Simpson emphasize that with prolonged second stage, continued pushing beyond 2-3 hours, and vertex at +3 station, the evidence-based next step is operative vaginal birth, provided prerequisites are met. Cesarean is not indicated when the fetal head is already low and deliverable vaginally.
AWHONN and Creasy & Resnik state that increasing oxytocin when facing fetal stress and prolonged second stage is contraindicated, because tachysystole worsens fetal oxygenation and increases risk of fetal compromise.
Exact Extract Concepts Referenced:
- "Expedited delivery is recommended when recurrent decelerations persist in second stage and the head is low enough for operative vaginal birth." (AWHONN Principles)
- "Oxytocin should be reduced or discontinued in the presence of nonreassuring patterns." (Simpson, Obstetric Interventions)
- "Operative vaginal delivery is appropriate with full dilation, engaged head, and prolonged second stage." (Menihan, Simpson; Creasy & Resnik)
NEW QUESTION # 62
A woman is being induced with oxytocin. The tracing shown is representative of 20 minutes. Based on this tracing, the next step would be to: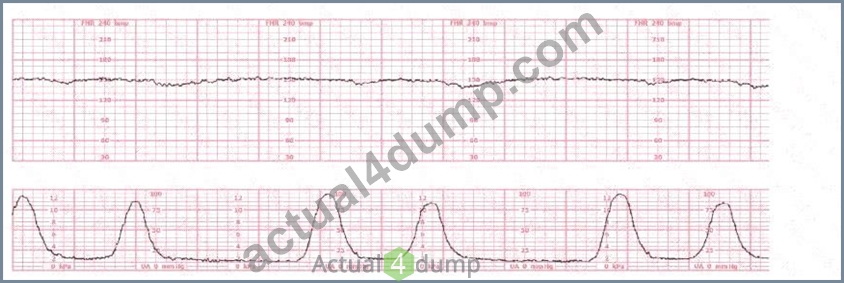
- A. Discontinue oxytocin
- B. Proceed to operative birth
- C. Place a spiral electrode
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
Evaluation of a tracing during oxytocin induction requires analysis of fetal status (baseline, variability, accelerations, decelerations) and uterine activity, with attention to tachysystole and fetal intolerance. NCC, AWHONN, Miller, Menihan, Simpson, and the NICHD guidelines all emphasize that oxytocin must be adjusted based on fetal response and contraction frequency.
Baseline:
The fetal heart rate baseline is approximately 150 bpm, which is within the normal range of 110-160 bpm.
Variability:
The tracing shows minimal variability (approximately 1-4 bpm amplitude). Minimal variability for a sustained period is categorized as a Category II pattern under NCC/NICHD classification.
Accelerations:
No accelerations are present during the 20-minute representative segment.
Decelerations:
There are no recurrent variable, no recurrent late, and no prolonged decelerations.
Uterine Activity:
The tracing shows very frequent contractions-approximately every 1½ to 2 minutes, which meets the NCC definition of tachysystole when averaged over 10 minutes (more than 5 contractions in 10 minutes).
According to NCC and AWHONN standards, when tachysystole is present with minimal variability, oxytocin must be reduced or discontinued even in the absence of late decelerations.
Clinical decision-making (per NCC principles):
NCC emphasizes that management of Category II patterns during induction starts with intrauterine resuscitative measures, including decreasing or stopping oxytocin when uterine activity is excessive or fetal response is suboptimal. Minimal variability with tachysystole requires correction of uterine stimulation before escalating to invasive monitoring or considering operative birth.
Option B (place a spiral electrode) is not indicated because the pattern is clearly visible and the priority is correcting uterine overstimulation, not refining the tracing.
Option C (operative birth) is not indicated; there is no Category III pattern or recurrent decelerations.
Option A (discontinue oxytocin) is the correct first-line action according to NCC-aligned guidelines when tachysystole and minimal variability occur.
References:
NCC C-EFM Candidate Guide (2025); NCC Content Outline; NICHD Three-Tier FHR Interpretation System; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 63
Accelerations that last 10 minutes or more are considered:
- A. Tachycardia
- B. Baseline variability
- C. A baseline change
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NICHD definitions endorsed by NCC:
* An acceleration lasting #10 minutes is no longer an acceleration
* It is classified as a baseline change
* This also applies to decelerations lasting #10 minutes being considered a new baseline bradycardia Why the incorrect answers are wrong:
* B. Baseline variability # refers to amplitude fluctuations, not duration.
* C. Tachycardia # requires baseline >160 bpm for 10 minutes, but the definition of "acceleration #10 minutes = baseline change" supersedes this.
References:NCC C-EFM Candidate Guide; NICHD Definitions; AWHONN FHMPP.
NEW QUESTION # 64
Fetal respiratory acidosis is most likely to present with which of the following fetal heart rate decelerations?
- A. Late
- B. Variable
- C. Early
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
NCC and AWHONN physiology teachings:
* Variable decelerations caused by cord compression lead to:
* Transient interruption of umbilical venous flow
* Impaired fetal gas exchange
* Acute rise in CO#
* Respiratory acidosis (early phase of hypoxemia)
This is well documented:
* Early decelerations # head compression # NOT associated with acidemia.
* Late decelerations # uteroplacental insufficiency # metabolic acidosis, not respiratory.
Thus:
* Variable decelerations # respiratory acidosis
* Late decelerations # metabolic acidosis
Correct answer: C. Variable
References:NCC Physiology Domain; AWHONN FHMPP; Menihan EFM; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 65
A woman at 41-weeks gestation is being induced. She is 2 cm dilated and is on oxytocin at 8 milliunits
/minute. Based on the fetal heart rate tracing shown, the best initial response is to: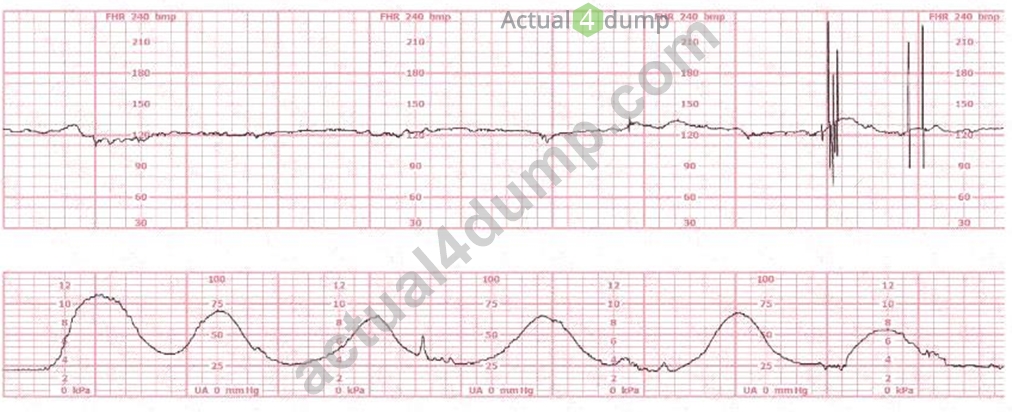
- A. Place a fetal spiral electrode
- B. Continue to observe
- C. Decrease the oxytocin
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
The tracing shows tachysystole with emerging late decelerations and minimal variability:
* 5 contractions in 10 minutes
* Deceleration nadirs occur after the peak of the contraction (late pattern)
* Variability begins to trend toward minimal
* The tracing has deteriorated while on oxytocin 8 mU/min, a common threshold for overstimulation NCC and AWHONN emphasize that when tachysystole occurs with any fetal intolerance, the first action is to reduce or stop oxytocin.
Key NCC principles:
* Late decelerations + tachysystole = uteroplacental insufficiency caused by excessive uterine activity
* Interventions:
* Stop or reduce oxytocin
* Maternal repositioning
* IV fluid bolus
* Possible oxygen if other measures fail
Why the other options are incorrect:
* A. Continue to observe - not acceptable with late decels + tachysystole.
* C. Place a spiral electrode - this corrects signal quality, not uterine overstimulation or fetal oxygenation.
Thus, the best initial response is B. Decrease the oxytocin.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; NICHD Definitions; Miller & Menihan EFM texts; Simpson & Creehan; Creasy & Resnik.
NEW QUESTION # 66
Maternal conditions of autoimmunity can result in fetal heart block due to antibodies that target:
- A. Fetal red blood cells
- B. The fetal atrioventricular node
- C. Maternal white blood cells
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
NCC physiology content specifically includes maternal autoimmune influences on fetal cardiac conduction.
Conditions such as maternal lupus (SLE) or Sjogren's syndrome may produce anti-Ro/SSA and anti-La
/SSB antibodies. These antibodies cross the placenta and damage fetal conduction tissue.
The primary site of injury is the fetal atrioventricular (AV) node, leading to:
* First-, second-, or complete third-degree heart block
* A slow, regular ventricular rate typically 50-70 bpm
* Loss of beat-to-beat variability because ventricular myocardium does not display normal autonomic modulation This mechanism is extensively described in AWHONN, NCC physiology materials, and maternal-fetal physiology texts.
Option A: Antibodies do not target fetal RBCs; that describes hemolytic disease of the newborn.
Option B: Targeting maternal WBCs is not fetal-specific.
The correct affected structure is the fetal AV node.
Therefore, the correct answer is C. The fetal atrioventricular node.
References:NCC C-EFM Candidate Guide (2025); NCC Physiology Content Outline; AWHONN Fetal Heart Monitoring Principles & Practices; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 67
This fetal heart rate tracing represents: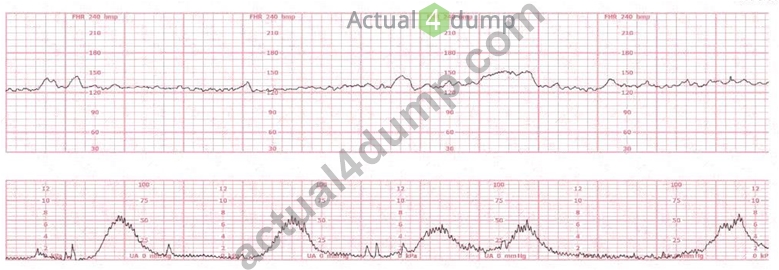
- A. Prolonged acceleration
- B. Coupling of contractions
- C. Category I tracing
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
The lower uterine tracing shows a repetitive contraction pattern characterized by pairs of contractions occurring close together, followed by a longer interval. This is known as "uterine contraction coupling." Key features confirming coupling:
* Two contractions occur back-to-back, separated by only a few seconds.
* Then a longer rest period occurs before the next pair.
* This pattern persists over several minutes.
* FHR remains normal with moderate variability and no decelerations.
Coupling is a uterine activity pattern, not a fetal heart rate abnormality.
Why the other answers are incorrect
A). Category I tracing
* While the FHR itself may appear reassuring, the question is explicitly about the pattern shown, which is (per NCC classification) a uterine pattern, not a category designation.
C). Prolonged acceleration
* A prolonged acceleration would be a fetal heart rate increase #15 bpm lasting #2 minutes but <10 minutes.
* No such FHR increase appears on the strip.
Thus, the correct interpretation is B. Coupling of contractions.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; Miller' s Pocket Guide; Menihan; Simpson & Creehan.
NEW QUESTION # 68
This patient received an epidural 15 minutes prior to the tracing shown. The next course of action is to: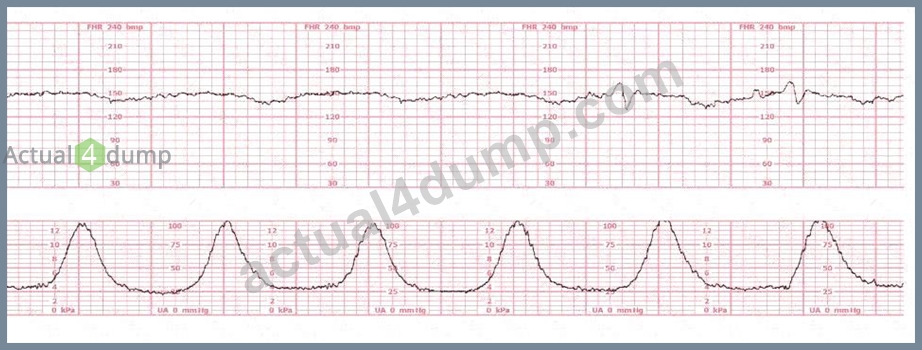
- A. Continue to monitor
- B. Check maternal blood pressure
- C. Perform a cervical exam
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
This tracing demonstrates:
* A sudden prolonged deceleration following epidural placement
* Minimal variability during the deceleration
* Event occurring within 15 minutes of epidural
NCC, AWHONN, and Menihan emphasize that maternal hypotension is the most common complication immediately following epidural analgesia. Hypotension leads to:
* Reduced uteroplacental perfusion
* Fetal bradycardia or prolonged decelerations
* Decreased variability during the deceleration
Typical fetal response to maternal hypotension:
Late-like or prolonged deceleration with weakening variability, exactly like the strip shown.
Therefore, the FIRST and most critical step is to check maternal blood pressure.
Other options:
* B. Continue to monitor - unsafe when a prolonged deceleration is present.
* C. Cervical exam - not indicated; the fetal tracing deterioration is temporally linked to epidural placement.
Thus, the correct action is A. Check maternal blood pressure.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; Menihan Electronic Fetal Monitoring; Miller's Fetal Monitoring Pocket Guide; Creasy & Resnik Maternal- Fetal Medicine.
NEW QUESTION # 69
A nulliparous woman at term presents with leaking fluid. Rupture of membranes confirmed. After 6 hours she is completely dilated, +2 station, has been pushing 2 hours with oxytocin at 10 mU/min. The fetal tracing is shown. What is the next step in management?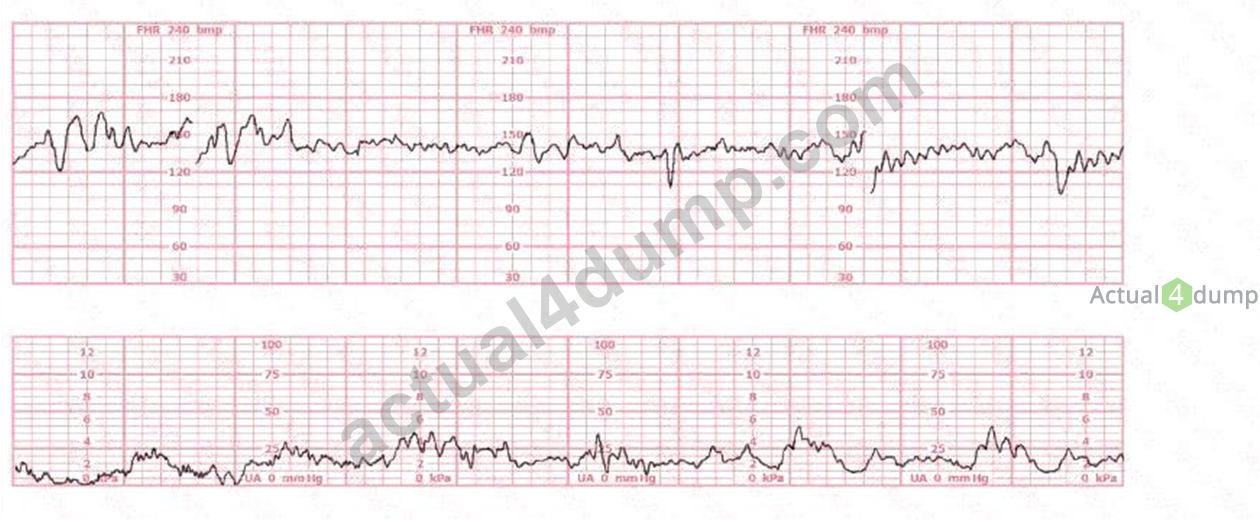
- A. Expedite birth
- B. Decrease oxytocin
- C. Continue pushing for another hour
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract Without Any URLs or Links:
According to the NCC C-EFM 2025 Exam Content Outline and recommended references such as AWHONN Fetal Heart Monitoring Principles, Simpson & Miller (Fetal Monitoring Text), and Menihan's EFM Guide, recurrent variable or late decelerations with minimal or moderate variability during the second stage of labor-particularly when the patient has been pushing for #2 hours-indicate progressive fetal intolerance of labor.
AWHONN states that when the fetal tracing displays recurrent variable decelerations with ongoing stress from long second stage, the recommended intervention is operative or expedited vaginal birth, provided the fetal station is at +2 or lower. AWHONN and Simpson emphasize that reducing oxytocin is insufficient when the tracing demonstrates ongoing significant decelerations during active pushing with adequate descent.
The NCC blueprint within Pattern Recognition & Intervention emphasizes:
* Identifying worsening recurrent decelerations
* Acting when fetal tolerance is decreasing
* Prioritizing timely intervention when the second stage exceeds standard limits with a non-reassuring tracing Because she is fully dilated, vertex at +2, and tracing shows recurrent decelerations during pushing, the evidence-based next step is expediting birth, typically via operative vaginal delivery.
References:AWHONN Fetal Heart Monitoring Principles & PracticesSimpson & Miller: Fetal MonitoringMenihan: Electronic Fetal MonitoringNCC C-EFM Exam Content Outline 2025
NEW QUESTION # 70
......
EFM Dumps for success in Actual Exam: https://www.actual4dump.com/NCC/EFM-actualtests-dumps.html
EFM Dumps Special Discount for limited time Try FOR FREE: https://drive.google.com/open?id=1AIHcBCZMloTIbi3_uWuAYGwIGvBOgwJ_